Anterior Pelvic Tilt, Is It A Problem?
The orientation and ‘biomechanics’ of the pelvis has been an area of deep interest in the movement and physical therapy world for decades. As the pelvis is the mediator between the spine and legs, the athrokinematics (joint) and osteokinematics (bone) have been thought to play a significant role in how ascending and descending forces are transferred throughout the body. Any small or large adjustments at the pelvis have the potential to influence the rest of the body either positively or negatively.
Many working theories about the pelvis and it’s influence on the rest of the body (especially the lower back) has inspired many modalities to focus on promoting the ‘correct’ pelvic posture and movement to encourage health, minimise or eliminate pain and to reduce the risk of pathology. As always there is little agreement on what is the appropriate level of ‘tilt’ at the pelvis or if any ‘tilt’ at all is the ideal pelvic position. It seems that allot of what is taught is based off someone’s opinion. There’s absolutely nothing wrong with having an opinion (I have plenty!) but what have researchers reported when comparing the pelvic posture of those with pain and those without pain?
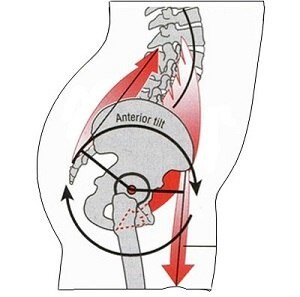
Anterior Pelvic Tilt
One study looked at 120 ‘healthy’ subjects (65 males and 55 females), measuring the resting position of their pelvis. All subjects were asymptomatic (1).
85% of males and 75% of females presented with an anterior pelvic tilt.
6% of males and 7% of females presented with a posterior pelvic tilt.
9% of males and 18% of females presented with a neutral pelvis.
Based off this study, roughly 75-85% of the population without pain present with an anterior pelvic tilt. This doesn’t mean that an anterior pelvic tilt doesn’t have the capacity to contribute to pain (back pain for example) but what we can interpret from this study is that an anterior pelvic tilt is ‘normal’ for most people. The next question might be, although an anterior pelvic tilt may be ‘normal’ for most people, is there a degree of anterior pelvic tilt that can increase the risk of pain or injury?
It’s been suggested that an anterior pelvic tilt of 12 degrees is ‘normal’ and potentially any degree of anterior rotation that exceeds that may put individuals at increase risk of pain or injury (2-3).
Lumbar Lordosis & Anterior Pelvic Tilt
One of the theories to why an anterior pelvic tilt may be an issue is that it creates more compression at the facet joints of the lumbar spine. Although the movements of the pelvis and lumbar spine are closely linked (rotating the pelvis changes the lordosis of the lumbar spine), studies haven’t found a strong correlation between the orientation of the pelvis and lumbar spine (4-7). This lack of correlation may be due to natural anatomical variations at pelvic girdles and so the orientation of the ASIS, PSIS and the lumbar spine may differ widely in individuals (8). These anatomical variations should always be acknowledged when considering the reliability and specificity of pelvic posture assessments in general.
Back Pain & The Pelvis
Although allot of studies haven’t found a meaningful connection to the posture of the pelvis and back pain, there are some studies that have found a ‘significant’ connection (9-10). What this might mean is for some, the alignment of the pelvis might contribute to back pain but for most people it likely isn’t a problem.
It is normal for the majority of the population to present with some degree for anterior pelvic tilt and it’s not necessarily and indication of muscle ‘imbalance’ or ‘weakness’ or incorrect alignment (11-13). Studies use different methods of pelvic assessment too which can also change the reliability of these findings in different papers.
What Does It All Mean?
If you have an anterior pelvic tilt (which you likely do to some degree) and you’re not in pain, don’t worry about it! Even if you have back pain it isn’t necessarily related to the orientation of the pelvis as there are many other factors that are more likely to contribute to back pain. As the movement of the pelvis influences the movement of the lumbar spine, promoting movement in all planes at the pelvis is prudent as lack of lumbar mobility has been associated with those suffering with lower back pain (as well as slow lumbar movement and poor proprioception). (14). It’s important to be aware that an anterior pelvic tilt isn’t a diagnosis and it’s only to explain the orientation of a pelvic girdle. Anterior rotation like any other position or movement of the pelvis is inherently fine. If an individual is habitually stuck in one position for long durations of time, this has the potential to over sensitise the surrounding tissues, leading to pain or discomfort. Although focusing on alignment may be useful for some pain individuals, for most a focus on strength and movement variability can be beneficial for maintaining pelvic/lower back health. Our pelvic posture is as unique as our fingerprints.
Want to learn new exercises and techniques to improve the health of the lower back based off the latest research on the fascia of the lower back?
Become a Franklin Method Lower Back Fascia Trainer (online certification). Click the link below to find out more:
Lower Back Fascia Trainer 9-11th Oct
Movement is medicine.
Tom
References
Assessment of the degree of pelvic tilt within a normal asymptomatic population. Lee Herrington 2011.
Effect of pelvic tilt on standing posture. J W Day. G L Smidt. T Lehmann. 1984.
Postural Aberrations in low back pain. H J Christie. S Kumar. S A Warren. 1995.
Relationship Between Mechanical Factors and Incidence of Low Back Pain. Mohammad Reza. Nourbakhsh, PT, PHD. Amir Massoud Arab, PT, MSc. 2012.
Relation Between Hip Extension Range of Motion and Postural Alignment. Jacklyn G. Heino, PT. Joseph J. Godges, PT, 0CS. Charles L. PhD, PT 1990.
Lumbar lordosis: study of patients with and without low back pain. Murrie VL1. Dixon AK. Hollingworth W. Wilson H. Doyle TA. 2003.
Relationships between lumbar lordosis, pelvic tilt, and abdominal muscle performance. Walker ML. Rothstein JM. Finucane SD. Lamb RL. 1987.
Variation in Pelvic Morphology May Prevent Identification of Anterior Pelvic Tilt. SJ Preece. 2008.
The Relation between Pelvic Tilt Angle and Disability Associated with Low Back Pain. Hee Sung Lim, PT, MS. Su Yeon RoH, PhD. Suk Min Lee, PT, DDS, PhD. 2012.
Relationship between mechanical factors and pelvic tilt in adults with and without low back pain. Krol A. Polak M. Szczygiel E. Wojcik P. Gleb K. 2017.
An Evaluation of Agonist: Antagonist Strength Ratios and Posture Among Powerlifters. Curtrufello, Paul T. Gadomski, Stephen J. Ratamess, Nicholas A. 2017.
Lumbar lordosis and pelvic inclination of asymptomatic adults. J W Youdas. T R Garrett. S Harmsen. V J Suman. J R Carey. 1996.
Lumbar lordosis and pelvic inclination in adults with chronic low back pain. J W Youdas. T R Garrett. K S Egan. T M Thereneau. 2000.
Comparing lumbo-pelvic kinematics in people with and without back pain: a systematic review and meta-analysis. Robert A Laird. Joyce Gilbert. Peter Kent. Jennifer L Keating. 2014.